Filter By
Associated Tasks
Demographics
AIDS Clinical Trials Group Study 175
| Classification+ | Tabular+ | 2.14k | 23 |
The AIDS Clinical Trials Group Study 175 Dataset contains healthcare statistics and categorical information about patients who have been diagnosed with AIDS. This dataset was initially published in 1996. The prediction task is to predict whether or not each patient died within a certain window of time or not.

Bone marrow transplant: children
| Classification+ | Multivariate | 187 | 36 |
The data set describes pediatric patients with several hematologic diseases: malignant disorders (i.a. acute lymphoblastic leukemia, acute myelogenous leukemia, chronic myelogenous leukemia, myelodysplastic syndrome) and nonmalignant cases (i.a. severe aplastic anemia, Fanconi anemia, with X-linked adrenoleukodystrophy). All patients were subject to the unmanipulated allogeneic unrelated donor hematopoietic stem cell transplantation. The motivation of the study was to identify the most important factors influencing the success or failure of the transplantation procedure. In particular, the aim was to verify the hypothesis that increased dosage of CD34+ cells / kg extends overall survival time without simultaneous occurrence of undesirable events affecting patients' quality of life (Kawłak et al., 2010). The data set has been used in our work concerning survival rules (Wróbel et al., 2017) and user-guided rule induction (Sikora et al., 2019). The authors of the research on stem cell transplantation (Kawłak et al., 2010) who inspired our study also contributed to the set.
CDC Diabetes Health Indicators
| Classification | Tabular+ | 253.7k | 21 |
Dataset link: https://www.cdc.gov/brfss/annual_data/annual_2014.html
Cirrhosis Patient Survival Prediction
| Classification | Tabular | 418 | 17 |
During 1974 to 1984, 424 PBC patients referred to the Mayo Clinic qualified for the randomized placebo-controlled trial testing the drug D-penicillamine. Of these, the initial 312 patients took part in the trial and have mostly comprehensive data. The remaining 112 patients didn't join the clinical trial but agreed to record basic metrics and undergo survival tracking. Six of these patients were soon untraceable after their diagnosis, leaving data for 106 of these individuals in addition to the 312 who were part of the randomized trial.

Diabetes 130-US hospitals for years 1999-2008
| Classification+ | Multivariate | 101.8k | 47 |
The dataset represents ten years (1999-2008) of clinical care at 130 US hospitals and integrated delivery networks. It includes over 50 features representing patient and hospital outcomes. Information was extracted from the database for encounters that satisfied the following criteria. (1) It is an inpatient encounter (a hospital admission). (2) It is a diabetic encounter, that is, one during which any kind of diabetes was entered into the system as a diagnosis. (3) The length of stay was at least 1 day and at most 14 days. (4) Laboratory tests were performed during the encounter. (5) Medications were administered during the encounter. The data contains such attributes as patient number, race, gender, age, admission type, time in hospital, medical specialty of admitting physician, number of lab tests performed, HbA1c test result, diagnosis, number of medications, diabetic medications, number of outpatient, inpatient, and emergency visits in the year before the hospitalization, etc.
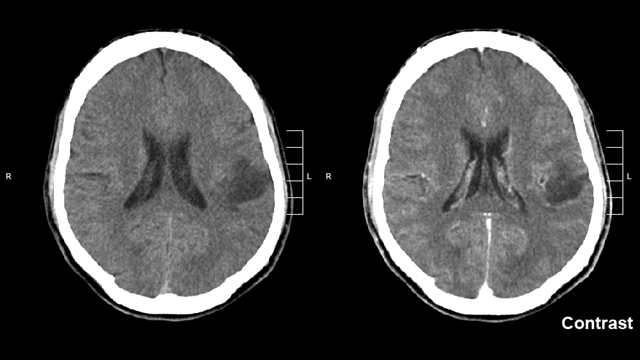
Glioma Grading Clinical and Mutation Features
| Classification+ | Tabular+ | 839 | 23 |
Gliomas are the most common primary tumors of the brain. They can be graded as LGG (Lower-Grade Glioma) or GBM (Glioblastoma Multiforme) depending on the histological/imaging criteria. Clinical and molecular/mutation factors are also very crucial for the grading process. Molecular tests are expensive to help accurately diagnose glioma patients. In this dataset, the most frequently mutated 20 genes and 3 clinical features are considered from TCGA-LGG and TCGA-GBM brain glioma projects. The prediction task is to determine whether a patient is LGG or GBM with a given clinical and molecular/mutation features. The main objective is to find the optimal subset of mutation genes and clinical features for the glioma grading process to improve performance and reduce costs.

HCV data
| Classification+ | Multivariate | 615 | 12 |
The target attribute for classification is Category (blood donors vs. Hepatitis C, including its progress: 'just' Hepatitis C, Fibrosis, Cirrhosis).
Heart Disease
| Classification | Multivariate | 303 | 13 |
This database contains 76 attributes, but all published experiments refer to using a subset of 14 of them. In particular, the Cleveland database is the only one that has been used by ML researchers to date. The "goal" field refers to the presence of heart disease in the patient. It is integer valued from 0 (no presence) to 4. Experiments with the Cleveland database have concentrated on simply attempting to distinguish presence (values 1,2,3,4) from absence (value 0). The names and social security numbers of the patients were recently removed from the database, replaced with dummy values. One file has been "processed", that one containing the Cleveland database. All four unprocessed files also exist in this directory. To see Test Costs (donated by Peter Turney), please see the folder "Costs"

Heart failure clinical records
| Classification+ | Multivariate | 299 | 12 |
A detailed description of the dataset can be found in the Dataset section of the following paper: Davide Chicco, Giuseppe Jurman: "Machine learning can predict survival of patients with heart failure from serum creatinine and ejection fraction alone". BMC Medical Informatics and Decision Making 20, 16 (2020). https://doi.org/10.1186/s12911-020-1023-5

ILPD (Indian Liver Patient Dataset)
| Classification | Multivariate | 583 | 10 |
This data set contains records of 416 patients diagnosed with liver disease and 167 patients without liver disease. This information is contained in the class label named 'Selector'. There are 10 variables per patient: age, gender, total Bilirubin, direct Bilirubin, total proteins, albumin, A/G ratio, SGPT, SGOT and Alkphos. Of the 583 patient records, 441 are male, and 142 are female. The current dataset has been used to study - differences in patients across US and Indian patients that suffer from liver diseases. - gender-based disparities in predicting liver disease, as previous studies have found that biochemical markers do not have the same effectiveness for male and female patients.
Infrared Thermography Temperature
| Regression | Tabular | 1.02k | 33 |
The Infrared Thermography Temperature Dataset contains temperatures read from various locations of inferred images about patients, with the addition of oral temperatures measured for each individual. The 33 features consist of gender, age, ethnicity, ambiant temperature, humidity, distance, and other temperature readings from the thermal images. The dataset is intended to be used in a regression task to predict the oral temperature using the environment information as well as the thermal image readings.

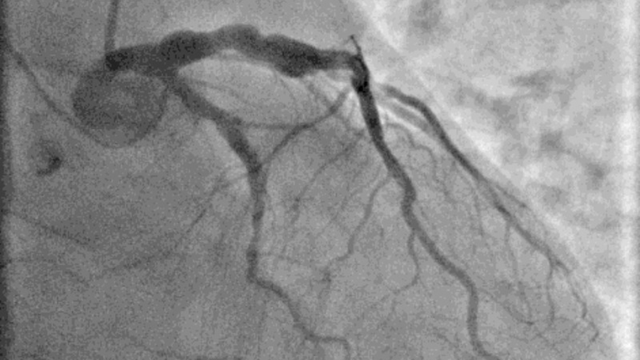
Myocardial infarction complications
| Classification | Multivariate | 1.7k | 111 |
Problems of real-life complexity are needed to test and compare various data mining and pattern recognition methods. The proposed database can be used to solve two practically important problems: predicting complications of Myocardial Infarction (MI) based on information about the patient (i) at the time of admission and (ii) on the third day of the hospital period. Another important group of tasks is phenotyping of disease (cluster analysis), dynamic phenotyping (filament extraction and identification of disease trajectories) and visualisation (disease mapping). MI is one of the most challenging problems of modern medicine. Acute myocardial infarction is associated with high mortality in the first year after it. The incidence of MI remains high in all countries. This is especially true for the urban population of highly developed countries, which is exposed to chronic stress factors, irregular and not always balanced nutrition. In the United States, for example, more than a million people suffer from MI every year, and 200-300 thousand of them die from acute MI before arriving at the hospital. The course of the disease in patients with MI is different. MI can occur without complications or with complications that do not worsen the long-term prognosis. At the same time, about half of patients in the acute and subacute periods have complications that lead to worsening of the disease and even death. Even an experienced specialist can not always foresee the development of these complications. In this regard, predicting complications of myocardial infarction in order to timely carry out the necessary preventive measures is an important task. Problems to solve In general columns 2-112 can be used as input data for prediction. Possible complications (outputs) are listed in columns 113-124. There are four possible time moments for complication prediction: on base of the information known at 1. the time of admission to hospital: all input columns (2-112) except 93, 94, 95, 100, 101, 102, 103, 104, 105 can be used for prediction; 2. the end of the first day (24 hours after admission to the hospital): all input columns (2-112) except 94, 95, 101, 102, 104, 105 can be used for prediction; 3. the end of the second day (48 hours after admission to the hospital) all input columns (2-112) except 95, 102, 105 can be used for prediction; 4. the end of the third day (72 hours after admission to the hospital) all input columns (2-112) can be used for prediction. You can find detailed description of database, descriptive statistics and csv version of database in DOI: 10.25392/leicester.data.12045261.v3
National Health and Nutrition Health Survey 2013-2014 (NHANES) Age Prediction Subset
| Classification | Tabular | 6.29k | 7 |
The original full dataset can be found at: https://wwwn.cdc.gov/nchs/nhanes/search/DataPage.aspx?Component=Questionnaire&CycleBeginYear=2013
National Poll on Healthy Aging (NPHA)
| Classification | Tabular | 714 | 14 |
This is a subset of the NPHA dataset filtered down to develop and validate machine learning algorithms for predicting the number of doctors a survey respondent sees in a year. This dataset’s records represent seniors who responded to the NPHA survey.

Parkinsons Telemonitoring
| Regression | Tabular | 5.88k | 19 |
This dataset is composed of a range of biomedical voice measurements from 42 people with early-stage Parkinson's disease recruited to a six-month trial of a telemonitoring device for remote symptom progression monitoring. The recordings were automatically captured in the patient's homes. Columns in the table contain subject number, subject age, subject gender, time interval from baseline recruitment date, motor UPDRS, total UPDRS, and 16 biomedical voice measures. Each row corresponds to one of 5,875 voice recording from these individuals. The main aim of the data is to predict the motor and total UPDRS scores ('motor_UPDRS' and 'total_UPDRS') from the 16 voice measures. The data is in ASCII CSV format. The rows of the CSV file contain an instance corresponding to one voice recording. There are around 200 recordings per patient, the subject number of the patient is identified in the first column. For further information or to pass on comments, please contact Athanasios Tsanas (tsanasthanasis@gmail.com) or Max Little (littlem@physics.ox.ac.uk). Further details are contained in the following reference -- if you use this dataset, please cite: Athanasios Tsanas, Max A. Little, Patrick E. McSharry, Lorraine O. Ramig (2009), 'Accurate telemonitoring of Parkinson’s disease progression by non-invasive speech tests', IEEE Transactions on Biomedical Engineering (to appear). Further details about the biomedical voice measures can be found in: Max A. Little, Patrick E. McSharry, Eric J. Hunter, Lorraine O. Ramig (2009), 'Suitability of dysphonia measurements for telemonitoring of Parkinson's disease', IEEE Transactions on Biomedical Engineering, 56(4):1015-1022
Regensburg Pediatric Appendicitis
| Classification | Tabular+ | 782 | 54 |
This dataset was acquired in a retrospective study from a cohort of pediatric patients admitted with abdominal pain to Children’s Hospital St. Hedwig in Regensburg, Germany. Multiple abdominal B-mode ultrasound images were acquired for most patients, with the number of views varying from 1 to 15. The images depict various regions of interest, such as the abdomen’s right lower quadrant, appendix, intestines, lymph nodes and reproductive organs. Alongside multiple US images for each subject, the dataset includes information encompassing laboratory tests, physical examination results, clinical scores, such as Alvarado and pediatric appendicitis scores, and expert-produced ultrasonographic findings. Lastly, the subjects were labeled w.r.t. three target variables: diagnosis (appendicitis vs. no appendicitis), management (surgical vs. conservative) and severity (complicated vs. uncomplicated or no appendicitis). The study was approved by the Ethics Committee of the University of Regensburg (no. 18-1063-101, 18-1063_1-101 and 18-1063_2-101) and was performed following applicable guidelines and regulations.

Sepsis Survival Minimal Clinical Records
| Classification | Multivariate | 110.3k | 3 |
Primary cohort from Norway: - 4 features for 110,204 patient admissions - file: 's41598-020-73558-3_sepsis_survival_primary_cohort.csv' Study cohort (a subset of the primary cohort) from Norway: - 4 features for 19,051 patient admissions - file: 's41598-020-73558-3_sepsis_survival_study_cohort.csv' Validation cohort from South Korea: - 4 features for 137 patients - file: 's41598-020-73558-3_sepsis_survival_validation_cohort.csv' The validation cohort from South Korea was used by Chicco and Jurman (2020) as an external validation cohort to confirm the generalizability of their proposed approach.
SUPPORT2
| Classification+ | Tabular+ | 9.11k | 42 |
Data sources are medical records, personal interviews, and the National Death Index (NDI). For each patient administrative records data, clinical data and survey data were collected. The objective of the SUPPORT project was to improve decision-making in order to address the growing national concern over the loss of control that patients have near the end of life and to reduce the frequency of a mechanical, painful, and prolonged process of dying. SUPPORT comprised a two-year prospective observational study (Phase I) followed by a two-year controlled clinical trial (Phase II). Phase I of SUPPORT collected data from patients accessioned during 1989-1991 to characterize the care, treatment preferences, and patterns of decision-making among critically ill patients. It also served as a preliminary step for devising an intervention strategy for improving critically-ill patients' care and for the construction of statistical models for predicting patient prognosis and functional status. An intervention was implemented in Phase II of SUPPORT, which accessioned patients during 1992-1994. The Phase II intervention provided physicians with accurate predictive information on future functional ability, survival probability to six months, and patients' preferences for end-of-life care. Additionally, a skilled nurse was provided as part of the intervention to elicit patient preferences, provide prognoses, enhance understanding, enable palliative care, and facilitate advance planning. The intervention was expected to increase communication, resulting in earlier decisions to have orders against resuscitation, decrease time that patients spent in undesirable states (e.g., in the Intensive Care Unit, on a ventilator, and in a coma), increase physician understanding of patients' preferences for care, decrease patient pain, and decrease hospital resource use. Data collection in both phases of SUPPORT consisted of questionnaires administered to patients, their surrogates, and physicians, plus chart reviews for abstracting clinical, treatment, and decision information. Phase II also collected information regarding the implementation of the intervention, such as patient-specific logs maintained by nurses assigned to patients as part of the intervention. SUPPORT patients were followed for six months after inclusion in the study. Those who did not die within six months or were lost to follow-up were matched against the National Death Index to identify deaths through 1997. Patients who did not die within one year or were lost to follow-up were matched against the National Death Index to identify deaths through 1997. All patients in five United States medical centers who met inclusion and exclusion criteria for nine disease categories: acute respiratory failure, chronic obstructive pulmonary disease, congestive heart failure, liver disease, coma, colon cancer, lung cancer, multiple organ system failure with malignancy, and multiple organ system failure with sepsis. SUPPORT is a combination of patients from 2 studies, each of which lasted 2 years. The first phase concerns 4,301 patients, whereas the second phase concerns 4,804 patients. Time wise, these studies were accessioned in 1989 (June 12) through 1991 (June 11) for phase I and in 1992 (January 7) through 1994 (January 24).
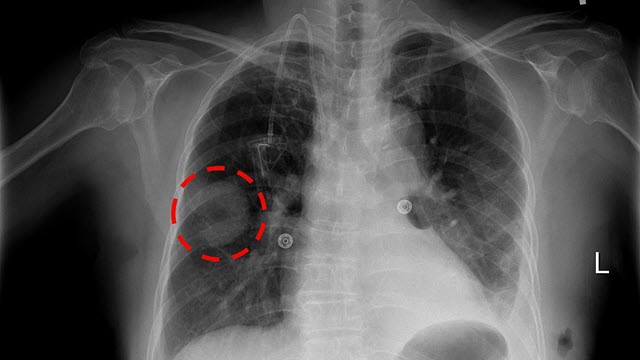
Thoracic Surgery Data
| Classification | Multivariate | 470 | 16 |
The data was collected retrospectively at Wroclaw Thoracic Surgery Centre for patients who underwent major lung resections for primary lung cancer in the years 2007 to 2011. The Centre is associated with the Department of Thoracic Surgery of the Medical University of Wroclaw and Lower-Silesian Centre for Pulmonary Diseases, Poland, while the research database constitutes a part of the National Lung Cancer Registry, administered by the Institute of Tuberculosis and Pulmonary Diseases in Warsaw, Poland.